

Dementia with Lewy bodies (DLB) is a progressive neurodegenerative disorder and one of the 2 clinical subtypes of Lewy body dementia (LBD), the other being Parkinson disease dementia (PDD). LBDs are characterized by the abnormal accumulation of α-synuclein, a protein found abundantly in neurons.1,2 In DLB, deposition of α-synuclein in the neocortex and limbic system leads to cognitive decline and a characteristic timeline of symptom onset.3,4 Cognitive symptoms, including visual hallucinations, typically precede or coincide with motor symptoms.2,5 Treatment focuses on symptom management, as no preventative or disease-modifying therapies currently exist.6
What is Dementia with Lewy bodies?
DLB is the second most common type of dementia after Alzheimer disease (AD).6,7 Prevalence remains uncertain due to small study sizes and diagnostic challenges.8 Most estimates suggest that DLB accounts for 3% to 7% of dementia diagnoses.6,8,9 DLB is more prevalent than PDD, making it the most common subtype of LBD.10 Unlike other dementias, DLB occurs more frequently in men than women.9,10 The mean age at onset is between 59 and 78 years.7
DLB is considered a sporadic disorder. However, genetic factors have been identified in 60% of cases.11 Duplications or mutations in SNCA, the gene that encodes α-synuclein, facilitate misfolding and aggregation.2,7 The apolipoprotein E (APOE) allele is also implicated, although its mechanism remains unclear.11,12 Other genes are associated with DLB, but they are less clinically relevant. Current research emphasizes epigenetic mechanisms contributing to the development of DLB.11
Pathophysiology
DLB is defined by the pathological accumulation of misfolded α-synuclein.1,2 In healthy neurons, α-synuclein modulates neurotransmitter release during synaptic transmission. It promotes neurotransmitter release by facilitating the formation of soluble N-ethylmaleimide-sensitive factor-attachment protein receptor (SNARE) complexes at the cell membrane. However, it also inhibits release through vesicle clustering. The physiologic structure of α-synuclein is an α-helix.3
In DLB, α-synuclein is misfolded. During the nucleation phase of protein formation, soluble monomers are bound together to form intermediate insoluble oligomers. During the elongation phase, the oligomers form primary filaments, and multiple primary filaments form fibrillar assemblies that organize into β-sheets.1 The β-sheets aggregate to form Lewy bodies (LBs) and Lewy neurites (LNs).2,3,13 Post-translational modification may influence regional heterogenicity in LB formation.2 Accumulation disrupts neurotransmitter release and causes neuronal death.3,4 Evidence supports prion-like propagation of α-synuclein across brain regions.2,7
LBs and LNs predominantly localize to the neocortex and limbic system, although the brainstem and subcortical regions may also be involved.2,6,7 Cell death in these regions alters cognitive functioning.2,6,7 Involvement of the substantia nigra leads to dopaminergic neuron loss.2
Making the Diagnosis
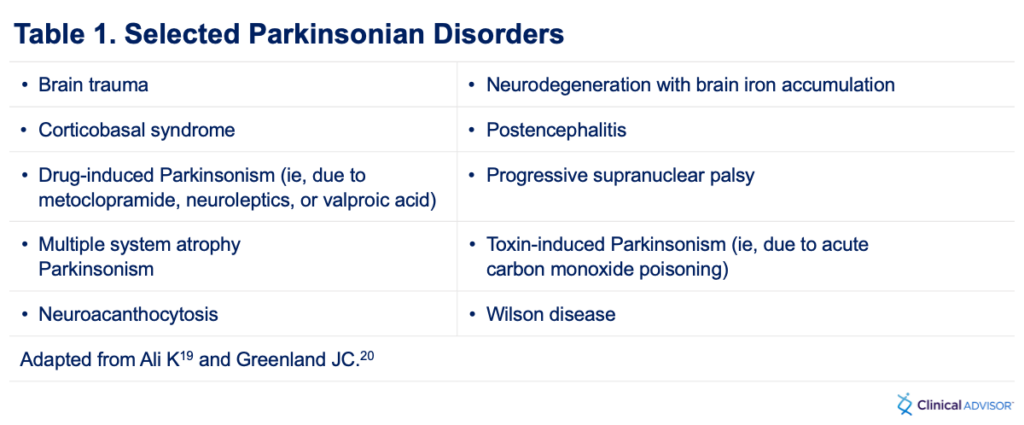
DLB may be misdiagnosed as other neurodegenerative or systemic diseases. The differential diagnosis includes AD, PDD, vascular dementia, normal pressure hydrocephalus (NPH), delirium, and other parkinsonian disorders (Table 1).2,14
Alzheimer’s Disease
AD involves the accumulation of extracellular amyloid-beta plaques and intracellular tau tangles that cause neuronal death. It is associated with slow onset and gradual progression of memory loss. Episodic memory loss is most common due to early involvement of the mesial temporal structures. Behavioral disturbances reflect changes in the frontal region. Other clinical manifestations include difficulty finding words, impaired facial recognition, and impaired reasoning.7 Visual hallucinations and extrapyramidal symptoms, common in DLB, are not typically present in AD.2,6,7
Parkinson’s Disease Dementia
PDD shares pathologic features with DLB, including the aggregation of α-synuclein into LBs and LNs.7 The key differentiator is timing.2,6,7 In PDD, cognitive symptoms and visual hallucinations emerge at least 1 year after the onset of motor symptoms such as rigidity, bradykinesia, masked facies, and shuffling gait.7 In DLB, cognitive decline, visual hallucinations, and motor symptoms occur concurrently or with cognitive symptoms preceding.2,6
Vascular Dementia
Vascular dementia is characterized by cognitive decline associated with cerebral infarcts. It involves loss of function occurring in a stepwise fashion along with focal neurologic abnormalities such as aphasia, hemiparesis, and spasticity. Parkinsonian features may also be seen. Imaging typically demonstrates ischemic changes,15 and clinical presentation varies based on the brain areas affected. Risk factors include hypertension, diabetes, hypercholesterolemia, cigarette smoking, and obesity.
Normal Pressure Hydrocephalus
NPH presents with the clinical triad of gait impairment, urinary incontinence, and cognitive dysfunction. The classic gait disturbance is described as a magnetic gait, because the feet appear to be stuck to the floor during ambulation. This may be confused with a parkinsonian gait. Imaging shows enlarged ventricles without significant brain atrophy. Lumbar puncture confirms normal cerebrospinal fluid pressure and may provide temporary symptomatic relief.16
Delirium
Delirium is a sudden change in mental status characterized by acute confusion, a fluctuating course, inattention, and sometimes hallucinations. It is common in older adults with cognitive dysfunction or dementia, particularly during hospitalization and in the presence of underlying illness or substance use. Delirium can be life-threatening and is associated with high rates of morbidity and mortality in this population. In cases of new or acute-onset visual hallucinations in individuals with preexisting dementia, a bedside screening tool such as the Confusion Assessment Method can help evaluate delirium. Potential causes of delirium are often multifactorial.17
Risk Factors for DLB
Nonmodifiable risk factors for DLB include age and family history.2,11 Risk increases substantially in individuals with a first-degree relative who has DLB, including a 2-fold increase if a sibling is affected.2 Depression and rapid eye movement sleep behavior disorder (RBD), characterized by acting out dreams through excessive extremity movement and shouting, are recognized risk factors.7,11 SNCA and APOE mutations are established genetic contributors.2,11 Low caffeine intake may increase risk, whereas cigarette smoking has not shown consistent effects.11
Clinical Presentations
DLB presents with progressive cognitive decline, often beginning with inattention and executive dysfunction.5 A hallmark feature is fluctuating cognition resembling delirium.2,6 Recurrent and well-formed visual hallucinations—often of children or animals—are highly characteristic. Of note, the presence of hallucinations can differentiate DLB from other forms of dementia, but the absence of hallucinations should not be used to rule out DLB.2,5,6 Although memory impairment is common, it typically progresses more slowly than in AD.2,6
Extrapyramidal motor symptoms such as resting tremor, rigidity, and bradykinesia typically develop later or alongside cognitive decline.2,5 Additional features include orthostatic hypotension and urinary incontinence.5 RBD is frequently observed and may precede other symptoms by up to 10 years.2,6
Diagnosis
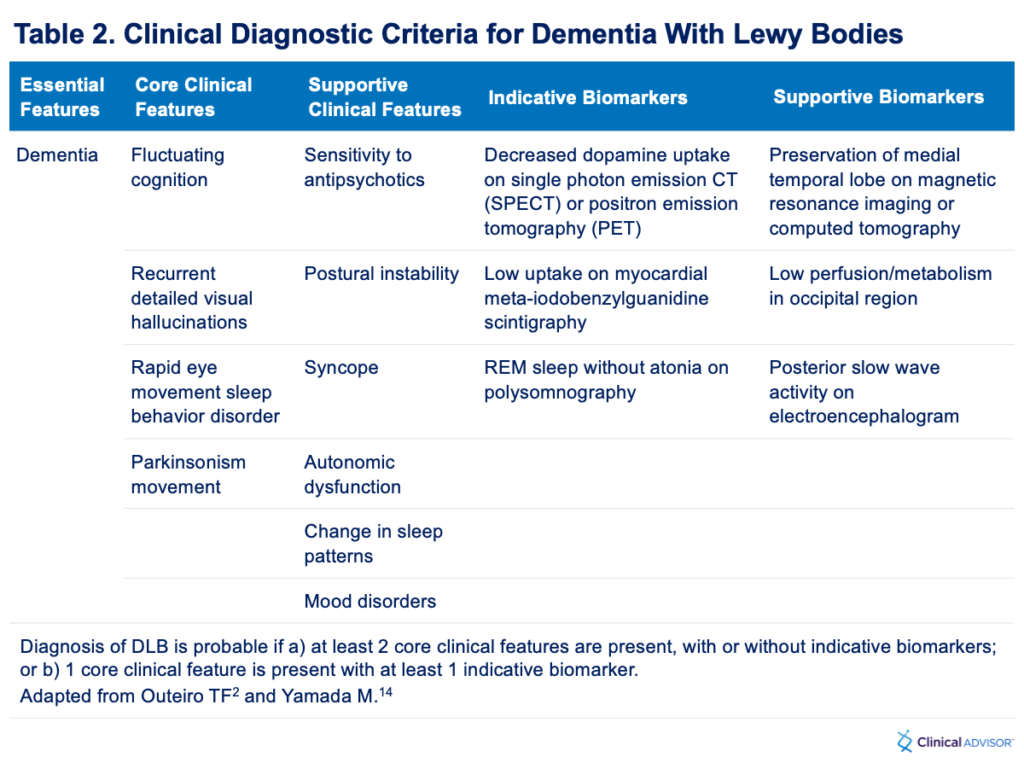
The diagnosis of DLB involves cognitive and movement assessments, polysomnography, imaging, and laboratory testing.2,6,7,18 Diagnostic criteria are sorted into essential, core, supportive, and indicative features (Table 2).19,20 Definitive diagnosis can only be made via postmortem biopsy confirming the presence of LBs and LNs.2,6,7,18
A DLB diagnosis requires evidence of dementia based on criteria in Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition, Text Revision. Cognitive impairment must affect at least 1 domain and interfere with daily function.5 Screening tools such as the Montreal Cognitive Assessment (MOCA) or the Mini-Mental Status Exam are commonly used, with MOCA preferred for early detection.6,18 Visual hallucinations may be evaluated using instruments like the North-East Visual Hallucination Interview.21
Movement assessments should be conducted by neurologists or movement disorder specialists. Relevant tools include the Movement Disorder Society Unified Parkinson’s Disease Rating Scale, which evaluates motor components through history and physical exam. Bradykinesia, rigidity, and resting tremor are findings consistent with DLB.18
Polysomnography is used to detect RBD by measuring eye movements, muscle activity, and electroencephalogram waveforms during sleep. REM sleep without atonia indicates RBD. The presence of RBD is a core feature of DLB and may present years before cognitive decline.2,7,18
Neuroimaging is used to support a suspected diagnosis of DLB. Positron emission tomography (PET) may reveal glucose hypometabolism in the medial temporal and occipital lobes2,22,23; dopamine transporter scans can identify reduced uptake in the basal ganglia18,24,25; and magnetic resonance imaging can help rule out other disorders.7 Imaging can be used to assess peripheral tissues as well. Meta-iodobenzylguanidine cardiac scans may demonstrate decreased uptake, reflecting loss of autonomic neurons.2,14
No specific laboratory studies can confirm a diagnosis of DLB. However, routine testing—such as complete blood count, comprehensive metabolic panel, thyroid function, and cobalamin levels—can help exclude potentially reversible causes of dementia. Additional tests may be considered depending on the clinical presentation.26 Biomarker research is ongoing, with efforts focused on measuring α-synuclein in peripheral and central nervous system tissues.2,14
Treatment of DLB
No disease-modifying therapies currently exist for DLB. Treatment involves symptom control and quality of life (QoL), typically via a multidisciplinary approach combining pharmaceuticals (all used off-label), physiotherapy, and psychosocial interventions.6
Pharmacologic Therapy
Acetylcholinesterase inhibitors, such as donepezil and rivastigmine, are first-line agents for the cognitive symptoms of DLB.6 Memantine, an N-methyl-D-aspartate receptor antagonist, may provide additional benefit.6 Dopaminergic medications like levodopa are occasionally used to treat extrapyramidal symptoms and improve movement, but may exacerbate psychiatric symptoms.7,27 Zonisamide, an anticonvulsant, showed improvement in motor symptoms without worsening cognitive function in phase 3 trials in Japan.28 Atypical antipsychotics may be considered for psychiatric features but should be used with extreme caution, or be avoided, because of the neuroleptic sensitivity seen in DLB and their potential to exacerbate motor symptoms.6,7 Melatonin is safe and well tolerated for RBD but may have variable efficacy.6 Clonazepam may reduce nocturnal movements associated with RBD but should be used with caution as it can increase risk for falls and worsen cognitive impairment.6
Physiotherapy
Physical, occupational, and speech therapy are essential components of supportive care and maintaining QoL in DLB. Physical therapy focuses on increasing muscle strength and balance to reduce gait disturbances. Occupational therapy supports greater independence by improving performance in activities of daily living (ADLs). Targeted speech therapy aims to preserve language function29 and assess risk for aspiration through swallowing tests. If aspiration risk is identified, modified diets may be recommended to ensure safe oral intake.
Psychosocial Interventions
Psychosocial interventions play a critical role in managing the behavioral and psychological symptoms of DLB, particularly to decrease agitation and risk for injury. Cognitive behavioral therapy and the recognition of visual hallucinations can help alleviate psychiatric symptoms. Music therapy has been shown to decrease agitation. Reorientation during episodes of cognitive fluctuation can lessen confusion and temporarily enhance cognitive performance but can also paradoxically increase agitation.30 A stable and familiar living environment is recommended to minimize disorientation, and a clean, uncluttered space can help reduce fall risk.6
Complications and Prognosis
DLB causes progressive decline in language, memory, attention, visuospatial perception, executive function, and social cognition, ultimately leading to loss of functional independence. As the ability to perform ADLs deteriorates, many individuals require in-home caregiving or admission to skilled nursing facilities.2,6 Mood changes ranging from agitation to depression are common.10,18 Worsening visual hallucinations often exacerbate stress, agitation, and confusion.6 DLB is also associated with various physical and autonomic complications. Aspiration pneumonia is the most common cause of hospitalization.10 Autonomic dysfunction can manifest as urinary incontinence, constipation, and orthostatic hypotension as the disease progresses and autonomic nerve fibers become involved.2,7 Falls tend to increase in frequency as motor symptoms worsen.6,18 RBD can result in injury from falling out of bed or hitting nearby objects during sleep.6
Research on the prognosis of DLB remains limited. However, overall, prognosis is considered worse when compared with other forms of dementia. DLB is associated with more rapid rates of cognitive decline and greater reduction in life expectancy.31 No disease-modifying medications are available, and reversal of LB and LN pathology is not possible. Although symptomatic treatments may offer temporary relief, they do not alter the underlying disease process.2,6,7 As the disease progresses, cognitive decline, motor dysfunction, and visual hallucinations typically worsen.31 Complications of dementia are the most commonly reported cause of death in individuals with DLB.29 Survival times vary widely, ranging from 2 to 20 years after diagnosis, with an average survival time of 6 years.31
Conclusion
DLB is characterized by the abnormal accumulation of α-synuclein into LBs and LNs. Core features include fluctuating cognition, visual hallucinations, RBD, and extrapyramidal motor symptoms. Movement disturbances typically manifest concurrently with or shortly after the onset of cognitive symptoms. Diagnosis is based mostly on clinical presentation and supported by imaging, although DLB is commonly misdiagnosed as another form of neurodegenerative dementia. Currently, no disease-modifying therapies exist. As a result, treatment requires a multifactorial approach to reducing symptoms and maintaining quality of life. Increased awareness of DLB is essential to improving diagnostic accuracy and encouraging further research into pharmaceutical interventions.
This article originally appeared on Clinical Advisor
References:
- Mehra S, Sahay S, Majir SK. α-Synuclein misfolding and aggregation: implications in Parkinson’s disease pathogenesis. Biochim Biophys Acta Proteins Proteom. 2019;1867(10):890-908. doi:10.1016/j.bbapap.2019.03.001
- Outeiro TF, Koss DJ, Erskine D, et al. Dementia with Lewy bodies: an update and outlook. Mol Neurodegener. 2019;14(5):1-18. doi:10.1186/s13024-019-0306-8
- Sharma M, Burré J. α-Synuclein in synaptic function and dysfunction. Trends Neurosci. 2023;46(2)153-166. doi:10.1016/j.tins.2022.11.007
- Mahul-Mellier AL, Burtscher J, Maharjan N, et al. The process of Lewy body formation, rather than simply α-synuclein fibrillization, is one of the major drivers of neurodegeneration. PNAS Nexus. 2020;117(9)4971-4982. doi:10.1073/pnas.1913904117
- Morenas-Rodríguez E, Sala I, Subirana A, et al. Clinical subtypes of dementia with Lewy bodies based on the initial clinical presentation. J Alzheimers Dis. 2018;64(2):505-513. doi:10.3233/JAD-180167
- Parish AL, Kim J. Clinical update on dementia with Lewy bodies for primary care NPs. Nurse Pract. 2023;48(4):22-29. doi:10.1097/01.NPR.0000000000000033
- Erkkinen MG, Kim MO, Geschwind MD. Clinical neurology and epidemiology of the major neurodegenerative diseases. Cold Spring Harb Perspect Biol. 2018;10(4):1-46. doi:10.1101/cshperspect.a033118
- Desai U, Chandler J, Kirson N, et al. Epidemiology and economic burden of Lewy body dementia in the United States. Curr Med Res Opin. 2022;38(7):1177-1188. doi:10.1080/03007995.2022.2059978
- Kane JP, Surendranathan A, Bentley A, et al. Clinical prevalence of Lewy body dementia. Alzheimers Res Ther. 2018;10(19):1-8. doi:10.1186/s13195-018-0350-6
- Forns J, Danysh HE, McQuay LJ, et al. Clinical outcomes and treatment patterns of older adults with dementia-related psychosis by dementia type in the United States. BMC Geriatr. 2022;22(784):1-10. doi:10.1186/s12877-022-03489-3
- Chouliaras L, Kumar GS, Thomas AJ, Lunnon K, Chinnery PF, O’Brien JT. Epigenetic regulation in the pathophysiology of Lewy body dementia. Prog Neurobiol. 2020;192:101822. doi:10.1016/j.pneurobio.2020.101822
- Gan J, Chen Z, Liu S, et al. The presence and co-incidence of geriatric syndromes in older patients with mild-moderate Lewy body dementia. BMC Neurol. 2022;22(355):1-11. doi:10.1186/s12883-022-02897-7
- Movalley. Immunostaining (brown) of alpha-synuclein in Lewy bodies and Lewy neurites in the neocortex of a patient with Lewy body disease. Wikimedia Commons. Revised September 20, 2020. Accessed June 12, 2025. https://commons.wikimedia.org/wiki/File:Immunostaining_(brown)_of_alpha-synuclein_in_Lewy_Bodies_and_Lewy_Neurites_in_the_neocortex_of_a_patient_with_Lewy_Body_Disease.jpg
- Yamada M, Komatsu J, Nakamura K, et al. Diagnostic criteria for dementia with Lewy bodies: updates and future directions. J Mov Disord. 2020;13(1):1-10. doi:10.14802/jmd.19052
- Khan A, Kalaria RN, Corbett A, Ballard C. Update on vascular dementia. J Geriatr Psychiatry Neuro. 2016;29(5):281-301. doi:10.1177/0891988716654987
- Passos-Neto CE, Lopes CC, Teixeira MS, Studart Neto A, Spera RR. Normal pressure hydrocephalus: an update. Arq Neuropsiquiatr. 2022;80(5)1:42-52. doi:10.1590/0004-282X-ANP-2022-S118
- Wilson JE, Mart MF, Cunningham C, et al. Delirium. Nat Rev Dis Primers. 2020;6(90)1-26. doi:10.1038/s41572-020-00223-4
- Matar E, Ehgoetz Martens KA, Halliday GM, Lewis SJG. Clinical features of Lewy body dementia: insights into diagnosis and pathophysiology. J Neurol. 2020;267(2):380-389. doi:10.1007/s00415-019-09583-8
- Ali K, Morris HR. Parkinson’s disease: chameleons and mimics. Pract Neurol. 2015;15(1):14-25. doi:10.1136/practneurol-2014-000849
- Greenland JC, Barker RA. The Differential Diagnosis of Parkinson’s Disease. In: Stoker TB, Greenland JC, eds. Parkinson’s Disease: Pathogenesis and Clinical Aspects. Brisbane, AU: Codon Publications; 2018. doi:10.15586/codonpublications.parkinsonsdisease.2018.ch6
- D’Antonio F, Boccia M, Di Vita A, et al. Visual hallucinations in Lewy body disease: pathophysiological insights from phenomenology. J Neurol. 2022;269(7):3636-3652. doi:10.1007/s00415-022-10983-6
- McKeith IG, Boeve BF, Dickson DW, et al. Fourth consensus report of the DLB Consortium. Neurology. 2017;9(1):88-100. doi:10.1212/WNL.0000000000004058
- McKeith IG, Boeve BF, Dickson DW, et al. Surface FDG Alzheimer disease and dementia with Lewy bodies. Wikimedia Commons. Revised June 29, 2022. Accessed June 12, 2025. https://commons.wikimedia.org/wiki/File:Surface_FDG_Alzheimer_Disease_and_Dementia_with_Lewy_Bodies.jpg
- Nichols KJ, Chen B, Tomas MB, Palestro CJ. Interpreting 123I–ioflupane dopamine transporter scans using hybrid scores. Eur J Hybrid Imaging. 2018;2(1):1-13. doi:10.1186/s41824-018-0028-0
- Nichols KJ, Chen B, Tomas MB, Palestro CJ. Fp-cit examples. Wikimedia Commons. Revised September 16, 2020. Accessed June 12, 2025. https://commons.wikimedia.org/wiki/File:Fp-cit_examples.jpg
- Arvanitakis Z, Shah RC, Bennett DA. Diagnosis and management of dementia: review. JAMA. 2019;322(16):1589-1599. doi:10.1001/jama.2019.4782
- Taylor JP, McKeith IG, Burn DJ, et al. New evidence on the management of Lewy body dementia. Lancet Neruol. 2020;19(2):157-159. doi:10.1016/S1474-4422(19)30153-X
- Murata M, Odawara T, Hasegawa K, et al. Effect of zonisamide on parkinsonism in patients with dementia with Lewy bodies: a phase 3 randomized clinical trial. Parkinsonism Relat Disord. 2020;76:91-97. doi:10.1016/j.parkreldis.2019.12.005
- Armstrong MJ. Lewy body dementias. Continuum. 2019;25(1):128-146. doi:10.1212/CON.0000000000000685
- Connors MH, Quinto L, McKeith I, et al. Non-pharmacological interventions for Lewy body dementia: a systematic review. Psychol Med. 2018;48(11):1749-1758. doi:10.1017/S0033291717003257
- Mueller C, Soysal P, Rongve A, et al. Survival time and differences between dementia with Lewy bodies and Alzheimer’s disease following diagnosis: a meta-analysis of longitudinal studies. Aging Res Rev. 2019;50:72-80. doi:10.1016/j.arr.2019.01.005
