
Lead author Nagy Mekhail, MD, PhD discusses the importance of neuromodulation, specifically a closed loop spinal cord stimulation system (SCS), for the management of chronic pain.

Lead author Nagy Mekhail, MD, PhD discusses the importance of neuromodulation, specifically a closed loop spinal cord stimulation system (SCS), for the management of chronic pain.

Spinal cord stimulation (SCS) with a closed-loop system that uses recorded evoked compound action potentials (ECAPs) is superior to a fixed-output, open-loop system for patients with chronic back and leg pain.

Many patients with craniofacial pain syndromes such as trigeminal neuralgia, cluster headache, and migraine have an adequate response to pharmacologic therapies.

When traditional oral analgesics no longer control pain, some physicians are turning to alternative drug delivery methods that provide pain relief while avoiding systemic adverse effects.

Off-label antidepressant use for chronic pain has increased in recent years in part as a result of the opioid epidemic and the need to reduce prescribing and use of opioids for chronic pain.

Interventional pain modalities provide alternative analgesia in patients who are intolerant of pharmacologic agents, have comorbidities that require multiple medications, or have pain refractory to oral medications.
Emerging findings suggest that cervical noninvasive vagus nerve stimulation using the gammaCore device may represent an option with efficacy comparable to that of surgically implanted cervical vagus nerve stimulation, with a lower risk for side effects.

A particular challenge in this population is the effective management of migraine during pregnancy and lactation while minimizing the risk for harm to the fetus.

Accurate diagnosis is essential to inform treatment strategy, particularly with headaches that may be secondary to a potentially life-threatening medical condition.

Approximately half of the 14% of Americans who have severe headache and migraine report having tried interventions such as meditation, yoga, and deep breathing exercises.

A 13-year-old boy is sent to the emergency department for evaluation of fever and headache that have been present for approximately 1 week.

Cluster headache and migraine are distinct primary headache disorders that are associated with substantial pain and disability.
Hemicrania continua, one of the trigeminal primary headaches, causes intense unilateral pain for ≥3 months.

People with migraines and comorbid mood disorders often need treatments that address both conditions, as well as management of sleep, stress, and lifestyle issues.
Geoffrey Littlejohn, MD, provides a clinical perspective on the pathophysiology of fibromyalgia and the role of neurogenic inflammation in the disease process.

Providing guidance to improve dietary behavior, which may include supplementation to achieve an optimal nutritional status, can contribute to improved control of fibromyalgia symptoms.

Experts discuss the symptoms and prevalence of neurological manifestations in Sjogren syndrome.

For individuals with migraine frequency of 4 to 14 episodes per month, prophylactic medications and analgesics are required.

There is a growing emphasis on provider responsibility with the increasing focus of the overprescribing of opioids.
The judicious use of caffeine as adjuvant therapy to over-the-counter pain relievers can improve or relieve pain for patients with migraine or tension-type headaches.

Although pharmacotherapy remains the standard strategy for migraine management, there are many patients for whom nonpharmacological approaches are indicated.

Although peripheral nerve decompression has been found to be effective in relieving some symptoms for burn patients, there is still some uncertainty.
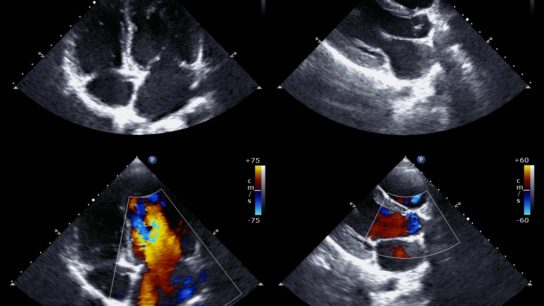
Despite mounting evidence suggesting the contrary, the debate on the potential benefits of patent foramen ovale closure for migraine is still ongoing.

The 2 treatments for cluster headache with Level A recommendations are either not readily accessible via public or private insurance or are not recommended in a large subset of patients with cardiovascular disease.

Despite a recent study concluding that oxygen therapy for cluster headache is not cost-prohibitive, many private payers and Medicare and Medicaid do not cover the effective therapy. Matthew Robbins, MD, Stewart Tepper, MD, and others weigh in on the controversial decision.
While several theories have evolved over the years, none have unequivocally provided robust evidence to fully explain the clinical spectrum of migraine.

Assessments showed a 66% reduction in pain during the session and a 33% reduction in pain at the end of the session.

Nearly 10% of pediatric patients with migraine also experience various episodic syndromes. Drs Amy Gelfand and Diana Lebron weigh in on what to look for to help you achieve the right diagnosis.

Multidisciplinary treatment may consist of psychological support and physical or occupational therapy along with the medical care provided by the referring physician.
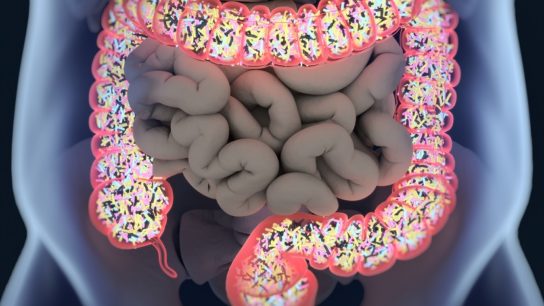
Nearly 10% of pediatric patients with migraine also experience various episodic syndromes involving gastrointestinal pain, vomiting, or vertigo.

You’ve read {{metering-count}} of {{metering-total}} articles this month.
We want you to take advantage of everything Neurology Advisor has to offer. To view unlimited content, log in or register for free.
{{login-button}} {{register-button}}
Want to view more content from Neurology Advisor?
Register now at no charge to access unlimited clinical news with personalized daily picks for you, full-length features, case studies, conference coverage, and more.
{{login-button}} {{register-button}}
Please login or register first to view this content.